8th Edition MCC Staging System Announced
October 13, 2016
Overview
As of January 2018, the AJCC 8th edition staging system will replace the 7th edition staging system. MCC patients will be categorized by their extent of disease at diagnosis (stage) as summarized in the 8th Edition table (see below) starting in 2017. The 2017 MCC staging system was based on an analysis of over 9,000 patients using the National Cancer Database as well as extensive review of the literature.1
There are two very important differences of the updated 8th edition staging system:
1) For the new system, it is important to designate if the stage was determined ‘clinically’ or ‘pathologically’. This has important implications in recurrence and survival. For example, if lymph nodes are only ‘clinically negative’ (doctors can not feel abnormal nodes on physical exam) this is less accurate than ‘pathologically negative’ nodes because microscopic MCC spread to nodes is present in one third of “clinically negative” nodes. Because ‘pathologically’ node negativity is thus more accurate, patients whose nodes are negative pathologically have a lower chance of experiencing a recurrence as compared to ‘clinically’ node negative patients because one third of these actually have early disease in their nodes.
2) Patients with nodal disease but no known primary tumor (‘unknown primary’) are now staged separately from patients that have nodal and a ‘known’ primary tumor. There are many studies that have shown that node-positive patients with an unknown primary tumor have an improved survival outcome compared to node-positive patients who have a visible tumor.234 For this reason, these two subtypes of stage III disease are separated.
Determining the 8th edition stage of Merkel cell carcinoma
MCC is divided into stages based on the primary tumor size and extent of disease (present in lymph nodes and or present at distant sites in the body). Furthermore, the 8th edition staging system is divided into how the disease was detected, either clinically or pathologically. Clinical stages can be determined by inspection, palpation of (feeling) the lymph nodes, or imaging studies. In contrast, pathological stages are based on microscopic study of tissue obtained by lymph node biopsy, or by needle biopsy.
The stage at diagnosis is the major determinant of the chance for later spread (metastasis) and treatment options.
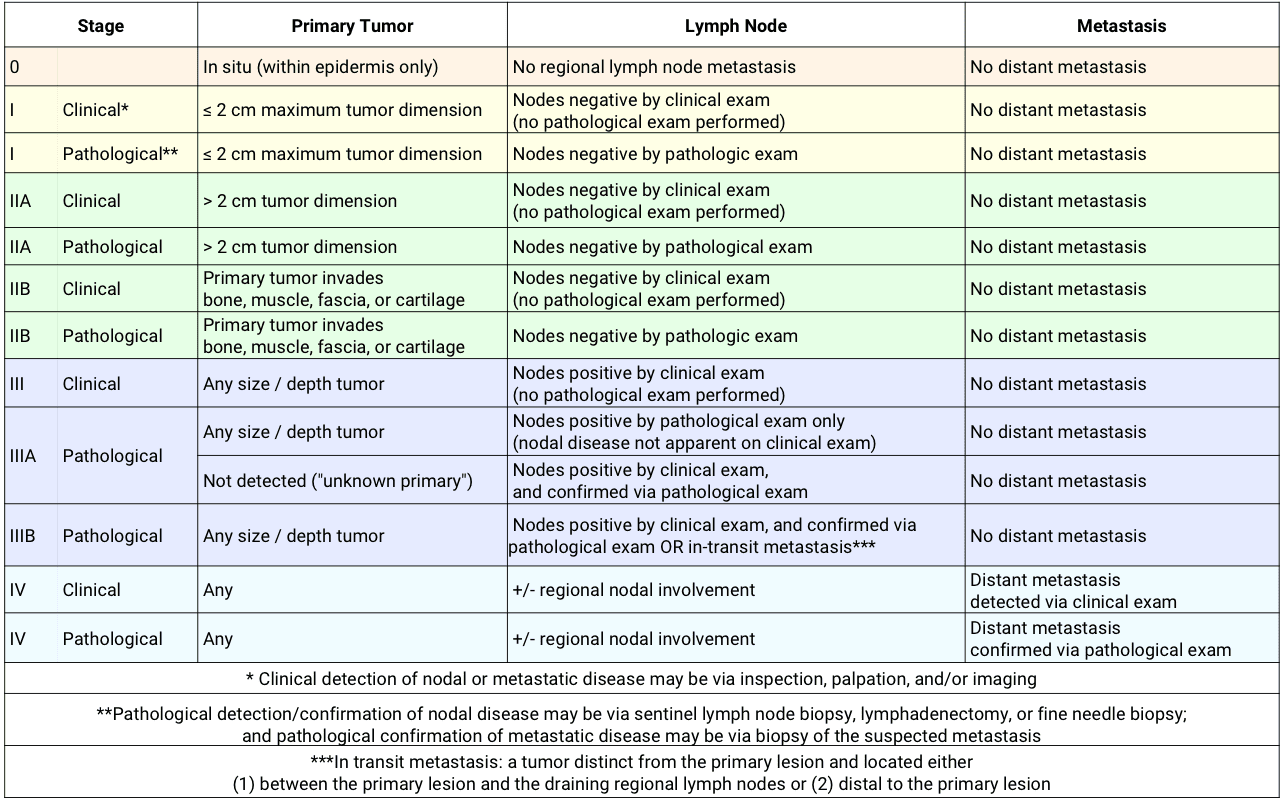
8th Edition MCC Staging Sytem Table
| Stage | Primary Tumor | Lymph Node | Metastasis | |
| 0 | In situ (within epidermis only) | No regional lymph node metastasis | No distant metastasis | |
| I | Clinical* | ≤ 2 cm maximum tumor dimension | Nodes negative by clinical exam (no pathological exam performed) |
No distant metastasis |
| I | Pathological** | ≤ 2 cm maximum tumor dimension | Nodes negative by pathologic exam | No distant metastasis |
| IIA | Clinical | > 2 cm tumor dimension | Nodes negative by clinical exam (no pathological exam performed) |
No distant metastasis |
| IIA | Pathological | > 2 cm tumor dimension | Nodes negative by pathological exam | No distant metastasis |
| IIB | Clinical | Primary tumor invades bone, muscle, fascia, or cartilage |
Nodes negative by clinical exam (no pathological exam performed) |
No distant metastasis |
| IIB | Pathological | Primary tumor invades bone, muscle, fascia, or cartilage |
Nodes negative by pathologic exam | No distant metastasis |
| III | Clinical | Any size / depth tumor | Nodes positive by clinical exam (no pathological exam performed) |
No distant metastasis |
| IIIA | Pathological | Any size / depth tumor | Nodes positive by pathological exam only
(nodal disease not apparent on clinical exam) |
No distant metastasis |
| Not detected (“unknown primary”) | Nodes positive by clinical exam,
and confirmed via pathological exam |
No distant metastasis | ||
| IIIB | Pathological | Any size / depth tumor | Nodes positive by clinical exam, and confirmed via pathological exam OR in-transit metastasis*** | No distant metastasis |
| IV | Clinical | Any | +/- regional nodal involvement | Distant metastasis detected via clinical exam |
| IV | Pathological | Any | +/- regional nodal involvement | Distant metastasis confirmed via pathological exam |
* Clinical detection of nodal or metastatic disease may be via inspection, palpation, and/or imaging
**Pathological detection/confirmation of nodal disease may be via sentinel lymph node biopsy, lymphadenectomy, or fine needle biopsy; and pathological confirmation of metastatic disease may be via biopsy of the suspected metastasis
***In transit metastasis: a tumor distinct from the primary lesion and located either (1) between the primary lesion and the draining regional lymph nodes or (2) distal to the primary lesion
Click here to download the 8th edition staging system.
{kind=link}
Understand the science
There are many studies that have shown that node-positive patients with an unknown primary tumor have an improved survival outcome compared to node-positive patients who have a visible tumor (Chen et al. 2013, Foote et al. 2011, and Tarantola et al. 2012). Several lines of evidence suggest that the reason for this is that the immune system eliminated the primary tumor in the ‘unknown primary’ cases, and the immune system is thus better able to eliminate other microscopic disease that may have spread elsewhere in the body.
What to do next
If a patient has just had an initial biopsy diagnosed as MCC, it is likely they can only be staged ‘clinically’. In most cases, a sentinel lymph node biopsy should be considered.
Footnotes
- 1Analysis of Prognostic Factors from 9387 Merkel Cell Carcinoma Cases Forms the Basis for the New 8th Edition AJCC Staging System. Harms KL, Healy MA, Nghiem P, Sober AJ, Johnson TM, Bichakjian CK, Wong SL. Ann Surg Oncol. 2016 Oct;23(11):3564-71. doi: 10.1245/s10434-016-5266-4. Epub 2016 May 19.
- 2A better prognosis for Merkel cell carcinoma of unknown primary origin. Chen KT, Papavasiliou P, Edwards K, Zhu F, Perlis C, Wu H, Turaka A, Berger A, Farma JM. Am J Surg. 2013 Nov;206(5):752-7. doi: 10.1016/j.amjsurg.2013.02.005. Epub 2013 Jul 5.
- 3 J Am Acad Dermatol. 2012 Sep;67(3):395-9. doi: 10.1016/j.jaad.2011.09.009. Epub 2011 Oct 26. Merkel cell carcinoma: the prognostic implications of an occult primary in stage IIIB (nodal) disease. Foote M1, Veness M, Zarate D, Poulsen M.
- 4 J Am Acad Dermatol. 2013 Mar;68(3):433-40. doi: 10.1016/j.jaad.2012.07.035. Epub 2012 Nov 19. Unknown primary Merkel cell carcinoma: 23 new cases and a review. Tarantola TI1, Vallow LA, Halyard MY, Weenig RH, Warschaw KE, Weaver AL, Roenigk RK, Brewer JD, Otley CC.