
Surgical excision
Jump to Section:
Purpose of surgical excision
The goal of surgical excision excision The removal of tissue of interest by surgery. for Merkel cell carcinoma Merkel cell carcinoma A skin cancer composed of cells that look microscopically similar to normal Merkel cells present in the skin. MCC was first described in 1972 and only in the 1990s was the CK20 antibody developed to make it easily identifiable by pathologists. Many doctors and patients are not aware of this cancer because of its recent description and relative rarity (~2,000 cases/year in the US--roughly 30 times less common than melanoma). About 40% of patients treated for MCC will experience a recurrence, making it far more aggressive than most other types of skin cancer, including melanoma. is to remove the Merkel cell Merkel cell Merkel cells are found in the lower part of the epidermis. Although the exact function of Merkel cells is unknown, they are thought to be touch receptors. Also known as neuroendocrine cells, they have machinery similar to nerve cells and to hormone-secreting (endocrine) cells. carcinoma carcinoma Cancer that originates in the skin or in the tissues lining the gut and ducts. so that it does not recur near the primary site primary site The area of the body where the abnormal tissue first appeared. or in the nearby lymph nodes. The primary MCC tumor should ideally be removed with clear margins (no microscopic tumor at edge of excision) as judged by pathology examination. As noted below however, when surgery is given alone (without any radiation) this can lead to a relatively high risk of MCC recurrence, up to 42%, depending on the study. The chance of local local Affecting only the site of origin, without evidence of spreading. Compare to systemic. recurrence after surgical excision of the primary tumor is far higher for MCC than for the more common types of skin cancer cancer A term used to describe diseases in which abnormal cells continually divide without normal regulation. Cancerous cells may invade surrounding tissues and may spread to other regions of the body via blood and the lymphatic system. ( basal cell carcinoma basal cell carcinoma Skin cancer that arises from basal cells, a cell type found in the innermost layer of the epidermis. Compared to other skin cancers, basal cell carcinoma is rarely lethal. Less than 1 in 50,000 patients with basal cell carcinoma will die from this disease. , squamous cell carcinoma squamous cell carcinoma Squamous cell carcinoma is a cancer that begins in squamous cells, which are thin, flat cells. Squamous cells are located in the middle layers of the epidermis, the lining of portions of the respiratory and digestive tracts, and the lining of some organs. Cutaneous squamous cell carcinoma affects about 100,000 Americans and has a mortality of roughly 2%. or even melanoma melanoma A form of skin cancer that begins in melanocytes (the skin cells that produce the pigment melanin). Melanoma affects about 42,000 Americans per year and has about a 15% mortality. ) because MCC more often “jumps” discontinuously to adjacent normal-appearing skin, with recurrences happening quite commonly up to several centimeters away from the primary tumor. The local recurrence rate can be as high as 20-40% depending on the study, and can typically be cut to less than 5% by the addition of radiation therapy radiation therapy The use of radiation to kill cancer cells and shrink tumors. Merkel cell carcinoma is a highly radiation sensitive cancer in most cases. . Importantly, if radiation will be used at the primary site, it is not required for the surgeon to obtain clear margins because radiation kills isolated tumor cells in the radiation field which usually extends at least 5 cm beyond where the tumor was. See the Radiation therapy page for guidelines about how to decide whether or not radiation should be used for a given patient.
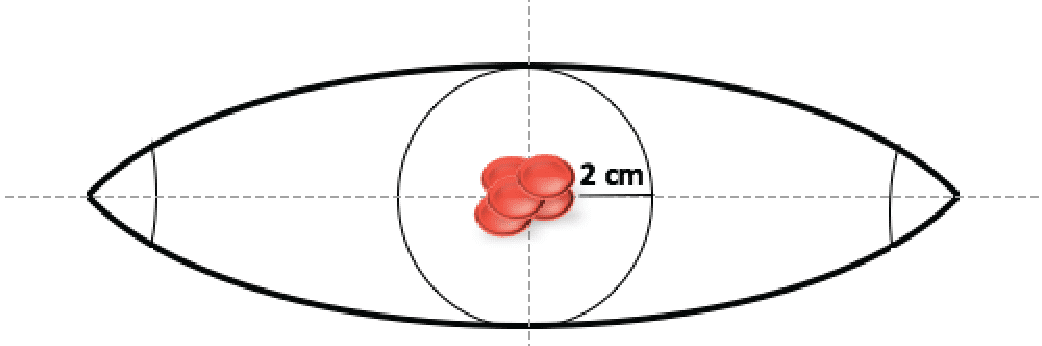
To optimize the appearance and function of the scar, the surgeon may make an excision in the shape of a football (ellipse). The length of the scar will be roughly three times the diameter of the excision around the tumor. (When possible, the excision is usually 2 cm beyond the tumor). Therefore, the scar may be up to eight times as long as the width of the original MCC tumor.
A Closer Look
In relatively low risk MCC tumors, surgery alone can be sufficient, as has been well documented especially by the groups at Memorial Sloan Kettering Cancer Center and University of Michigan.3 4 Among a large series of cases from the literature, the addition of adjuvant radiation to surgery decreased the risk of local recurrence by several fold.
Who this works for
Most patients will benefit from at least a narrow excision of their primary tumor that removes all of the tumor that can be readily felt or seen.
Who this doesn’t work for
Depending on your general health and the location and size of the MCC, surgery may not be possible. In such cases, radiation therapy is sometimes used alone and often has excellent outcomes.1, 2
Side effects
Surgical excision side effects are highly dependent on the location and size of the tumor and they mostly relate to how much skin needs to be excised near the tumor.
Often used in conjunction with
Radiation therapy of the area that was excised is often given to lower the risk of recurrence at the surgical site.
What to do next
After surgery is done, the pathology results should be reviewed by your team to determine whether or not radiation should be added. If not already performed, a baseline scan, ideally a PET/ CT scan CT scan A series of detailed 3-dimensional pictures of areas inside the body, taken from different angles; the pictures are created by a computer linked to an x-ray machine. Also called computerized axial tomography scan, computed tomography scan, CT scan, and computerized tomography. Contrast dye may be injected or taken orally to aid in accurately interpreting where in the body lesions occur. , is typically indicated. As soon as possible, an oncoprotein antibody titer antibody titer An antibody titer reflects the amount of a particular antibody in the blood. should be checked.
FAQs
What is the correct surgical margin size for a Merkel cell carcinoma?
This is an extremely tricky and controversial point. If radiation will be used, then surgical margins can be very small and narrow (just taking out the obvious portion of the tumor provides superb results when combined with adjuvant radiation). In contrast, if radiation is not planned, margins that are greater than 1 cm (ideally 2 cm) are associated with a lower risk of recurrence.
When is surgery alone sufficient for treating Merkel cell carcinoma (no radiation)?
This is an extremely controversial area. Some studies, including ones led by the Bichakjian and Coit teams, suggest that MCCs can be treated with surgery alone, with very few patients experiencing relapse. Other studies suggest that radiation cuts the risk of local recurrence by 2-3 fold. A reasonable approach is that surgical excision alone is likely sufficient for certain low-risk tumors. For example, no radiation is usually needed if the tumor is relatively small (<2cm), the sentinel lymph node biopsy is negative, larger surgical excision margins are achieved (typically about 2cm), there is no lymphovascular invasion noted by the pathologist, if the pathologist cannot find any tumor cells at the margin, and if the patient is not immune suppressed. If these higher risk factors are present, it means there would likely be greater benefit of adding radiation therapy.
When should the sentinel lymph node biopsy performed?
It is important to perform a sentinel lymph node biopsy at the time of (or prior to) a significant re-excision surgery. This is because extensive surgery at the site of the tumor disrupts the tiny lymphatic vessels that connect the tumor to the regional 1-2 lymph nodes where the cancer may have spread microscopically.
Do I need surgery?
A surgical excision is usually performed after a diagnostic biopsy as the first step of appropriate treatment for MCC. The goal of surgery is to remove any remaining cancer that can be seen either by the naked eye or under a microscope.
Footnotes
- 1 Pape E, Rezvoy N, Penel N, et al. Radiotherapy alone for Merkel cell carcinoma: a comparative and retrospective study of 25 patients. J Am Acad Dermatol. 2011;65(5):983-990. doi:10.1016/j.jaad.2010.07.043
- 2 Veness M, Howle J. Radiotherapy alone in patients with Merkel cell carcinoma: the Westmead Hospital experience of 41 patients. Australas J Dermatol. 2015;56(1):19-24. doi:10.1111/ajd.12263
- 3 Frohm ML, Griffith KA, Harms KL, et al. Recurrence and Survival in Patients With Merkel Cell Carcinoma Undergoing Surgery Without Adjuvant Radiation Therapy to the Primary Site. JAMA Dermatol. 2016;152(9):1001-1007. doi:10.1001/jamadermatol.2016.1428
- 4Fields RC, Busam KJ, Chou JF, et al. Recurrence after complete resection and selective use of adjuvant therapy for stage I through III Merkel cell carcinoma. Cancer. 2012;118(13):3311-3320. doi:10.1002/cncr.26626