Merkel cell polyomavirus is more frequently present in North American than Australian Merkel cell carcinoma tumors
January 1, 2009
Full Publication
TO THE EDITOR
Merkel cell carcinoma (MCC) is an increasingly common neuroendocrine cancer of the skin. MCC is an aggressive malignancy that is a significant cause of non-melanoma skin cancer deaths. Although the genetics of MCC are poorly characterized, it is well established that MCC is associated with advanced age and ultraviolet-light exposure. MCC is also linked to immune suppression; 8% of MCC patients are chronically immunosuppressed, which is a 16-fold over-representation(Heath et al., 2008). In particular, MCC is linked to T cell dysfunction associated with malignant, infectious and iatrogenic causes(Heath et al., 2008),(Engels et al., 2002),(Miller and Rabkin, 1999).
Recently, Feng et al. described a novel polyomavirus that is associated with Merkel cell carcinoma(Feng et al., 2008). This virus, named Merkel cell polyomavirus (MCPyV), was present in 8 of 10 MCC tumors as compared to 1 of 15 normal skin controls. Several clues suggest a possible functional role for this virus in cancer. MCPyV shares key features with the SV40 polyomavirus, an oncogenic virus in animals, such as the predicted ability of a viral protein to bind and inactivate the tumor suppressor Rb. Furthermore, MCPyV DNA was reported to be monoclonally integrated into six of the tumors, which implies that viral integration was an early event in MCC carcinogenesis and occurred before tumor expansion.
To confirm this recent discovery, we used quantitative real-time PCR to detect the presence or absence of Merkel cell polyomavirus DNA in 37 MCC tumor specimens originating from 37 patients in North America and Australia. Two primer sets targeting MCPyV, but not other known human polyomaviruses, were used. One set amplifies the region corresponding to the common portion of large and small T antigen (nucleotides 236–374 of the “MCV350” sequence, [EU375803]) and the second set amplifies a portion of the large T antigen surrounding a BamH1 restriction site (nucleotides 1083–1181). Products of the second set were digested with BamH1 and resolved on an acrylamide gel to verify product specificity. For a comparison control gene, primers were designed to amplify a gene on chromosome 2 (the TPO gene) because chromosome 2 is usually stable and only rarely gained or lost in MCC tumors(Van Gele et al., 1998). Serial dilutions were employed to calibrate the relative efficiency of the PCR reactions and ensure that the delta-delta CT method could be used to determine relative amounts of DNA between the viral and control genomic targets. The sensitivity of the real-time platform allowed us to detect levels of the viral gene as low as one five-thousandth the level of the control gene. All reactions were done in triplicate, and water and pooled human male lymphocyte DNA were included as negative controls. We also performed the PCR under less stringent conditions (lower annealing temperature). Under these conditions, we did not detect additional MCPyV positive tumors, but cannot rule out the possibility of presence of a strain variant in the negative tumors.
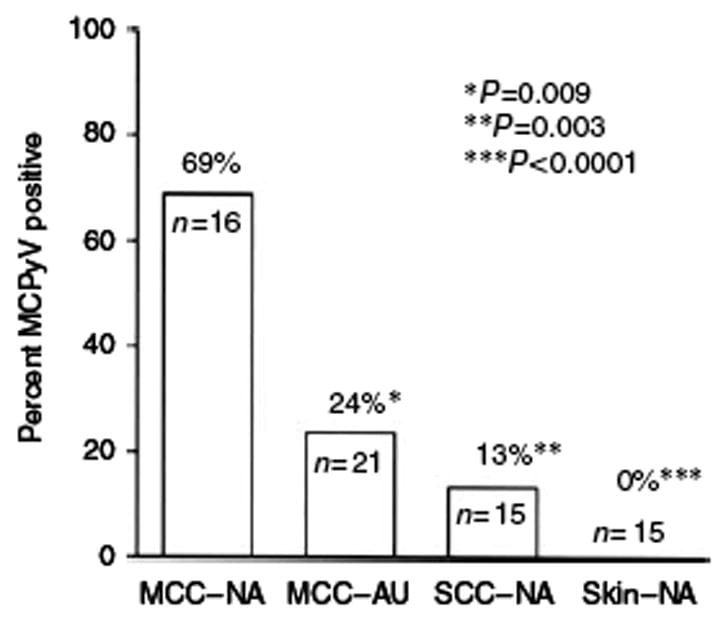
We found that 16 of 37 Merkel cell carcinoma tumor tissues were positive for Merkel cell polyomavirus DNA (43%). Interestingly, the proportion of tumors positive for MCPyV was much higher in tumors originating from North America than those originating from Australia (Figure 1). Among North American MCC specimens, 11 of 16 tumors (69%) were positive, which is similar to the initial report of 8 of 10 tumors(Feng et al., 2008). In contrast, only 5 of 21 Australian MCC specimens (24%) were positive for MCPyV. Additionally, we tested 15 primary squamous cell carcinoma (SCC) tumors, and 15 apparently normal sun-exposed skin samples, from 30 North American patients without MCC. These patients had a similar age and gender distribution to the MCC patients. MCPyV was not detected in any of the normal skin DNA, but was present in 2 of 15 SCC tumors (13%).
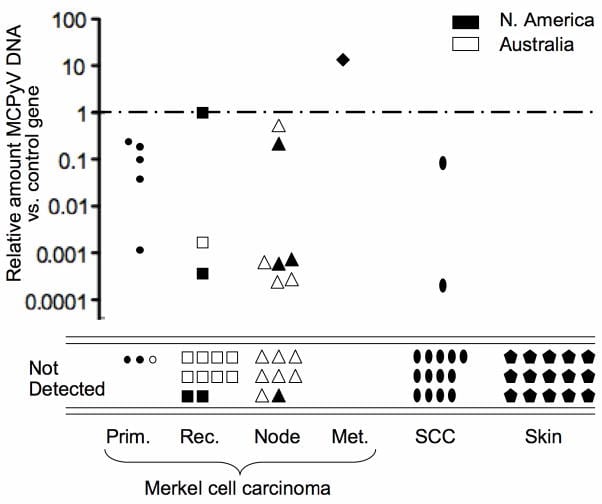
The MCC tumor tissues tested included primaries and metastases. We observed MCPyV in 5 of 8 primary tumors, 3 of 13 recurrences, 7 of 15 nodal metastases, and in the single studied distant metastasis. Outcome data were available for 30 of the 37 patients. In this subset, no survival difference was noted between virus positive and virus negative tumors using Kaplan-Meier analysis (data not shown). We found wide variation in the amount of viral DNA present. Indeed, the amount of viral DNA relative to control DNA varied over five orders of magnitude among the virus-positive MCC tumors (Figure 2).
Our data further present the interesting observation that North American MCC tumors are more frequently MCPyV positive than Australian MCC tumors. This difference may be due to the increased sun exposure in Australia, making a possible viral contribution less frequent. We cannot exclude the possibility that a different and unknown MCPyV strain, not detectable with our specific assay, or perhaps an alternate virus is present in the Australian Merkel cell carcinomas. The majority of Australian samples were nodal metastases, whereas most North American samples were primaries. However, we believe this is unlikely to account for our observed difference because for two North American tumors both primary and nodal tissues were available, and for each tumor both the primary and nodal tissues were similarly virus positive (data not shown). It is important to note that most of the Australian tumor specimens were collected in the 1990’s and most North American specimens were collected after the year 2000. However, DNA quality from the Australian specimens was excellent both by spectrophotometry and PCR of control genes. Our observed percentages may over- or under-represent the true prevalence of MCPyV in MCC tumors because our left-over surgical specimens are biased towards more advanced Merkel cell carcinoma than average. This was true of both the Australian and North American specimens.
2 of 15 SCC samples had detectable MCPyV DNA. A larger study is required to determine whether MCPyV is reproducibly more often present in SCC tumors than in normal skin.
Merkel cell polyomavirus represents an exciting direction for future studies in two major areas. The first area is functional characterization of the Merkel cell polyomavirus and determination if it expresses biologically active viral proteins and whether it is in fact involved in the generation or maintenance of MCC tumors. The second major direction is an epidemiologic characterization of the prevalence of MCPyV in healthy people and in various tumors as this virus may plausibly be associated with other human diseases or malignancies.
Footnotes
- 1Engels EA, Frisch M, Goedert JJ, Biggar RJ, Miller RW. Merkel cell carcinoma and HIV infection.Lancet. 2002;359:497–498.
- 2Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science. 2008;319:1096–1100.
- 3Heath M, Jaimes N, Lemos B, Mostaghimi A, Wang LC, Penas PF, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol.2008;58:375–381.
- 4Miller RW, Rabkin CS. Merkel cell carcinoma and melanoma: etiological similarities and differences. Cancer Epidemiol Biomarkers Prev. 1999;8:153–158.
- 5Van Gele M, Speleman F, Vandesompele J, Van Roy N, Leonard JH. Characteristic pattern of chromosomal gains and losses in Merkel cell carcinoma detected by comparative genomic hybridization. Cancer Res. 1998;58:1503–1508.